
5-Minute Lumbar
Triage Protocol —
The Clarity Imaging
Can't Give You.
Most non-specific LBP walks into your office without a clear mechanical diagnosis. This tool gives you one — in five minutes, at the point of care, with no additional equipment. Designed for primary care use.
Three Clinical Documents. One Package.
Every item is peer-reviewed, evidence-aligned, and ready to use at the point of care. The package is designed to reduce your back pain appointment time without reducing clinical rigour.
The 5-Minute Triage Checklist
Two pages. Every decision point covered. Red flags, mechanical pattern, neural involvement, SI joint, hip contribution — documented before the patient leaves your office.
2-page fillable clinical checklist · Decision summary includedWhy Your Patient Stopped Googling
Three pages. Patient handbook. They leave with a framework for their pain instead of a diagnosis they found at 2am.
3 pages · Plain language · Print-readyThe Evidence Behind the Conversation
14 citations. NEJM, Lancet, ACP. A claim-to-evidence map so you can verify every statement in the handout in under two minutes.
14 citations · Claim-to-evidence map · PubMed indexedWhy a Mechanical Screen — Before Imaging
These are the findings your patients are presenting with — regardless of their primary complaint — and why imaging often creates more clinical complexity than it resolves.
"Imaging labels — degeneration, herniation — increase fear, reduce movement, and slow recovery in patients who have no structural pathology requiring intervention."
Darlow et al., Ann Fam Med 2012 · Moseley & Butler, J Pain 2015
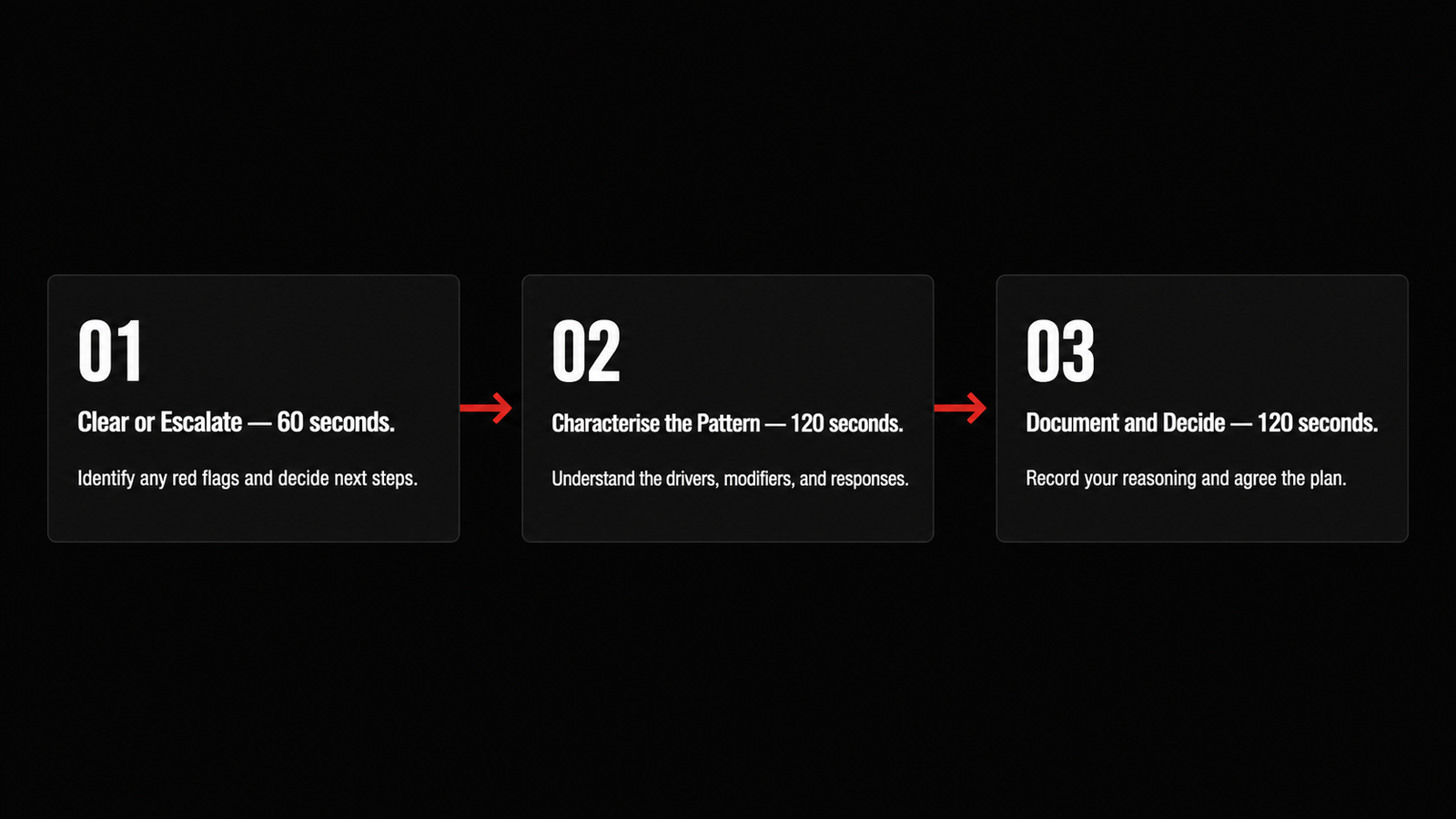
Three Phases. Five Minutes. One Documented Decision.
The tool runs in sequence during your standard physical examination block — no devices, no additional time slot required. It outputs a documented clinical impression before the patient leaves your office.
The Failure of Static Imaging in Functional LBP
Traditional spinal imaging captures structure, not function. While valuable for ruling out red-flag pathologies, static templates consistently miss the moving joint dynamics that drive mechanical low back pain.
The MRI Illusion
Up to 85% of chronic low back pain cases are classified as non-specific because static imaging cannot capture the movement patterns that drive pain. The scan shows where the tissue is stressed — it cannot show why the loading pattern keeps stressing it.
The Compensatory Loop
A patient's pain is rarely located where the actual mechanical fault lives. Degenerative changes on a scan are frequently the downstream result of a silent loading dysfunction elsewhere in the kinetic chain — identified in five minutes of movement testing, invisible on every image.
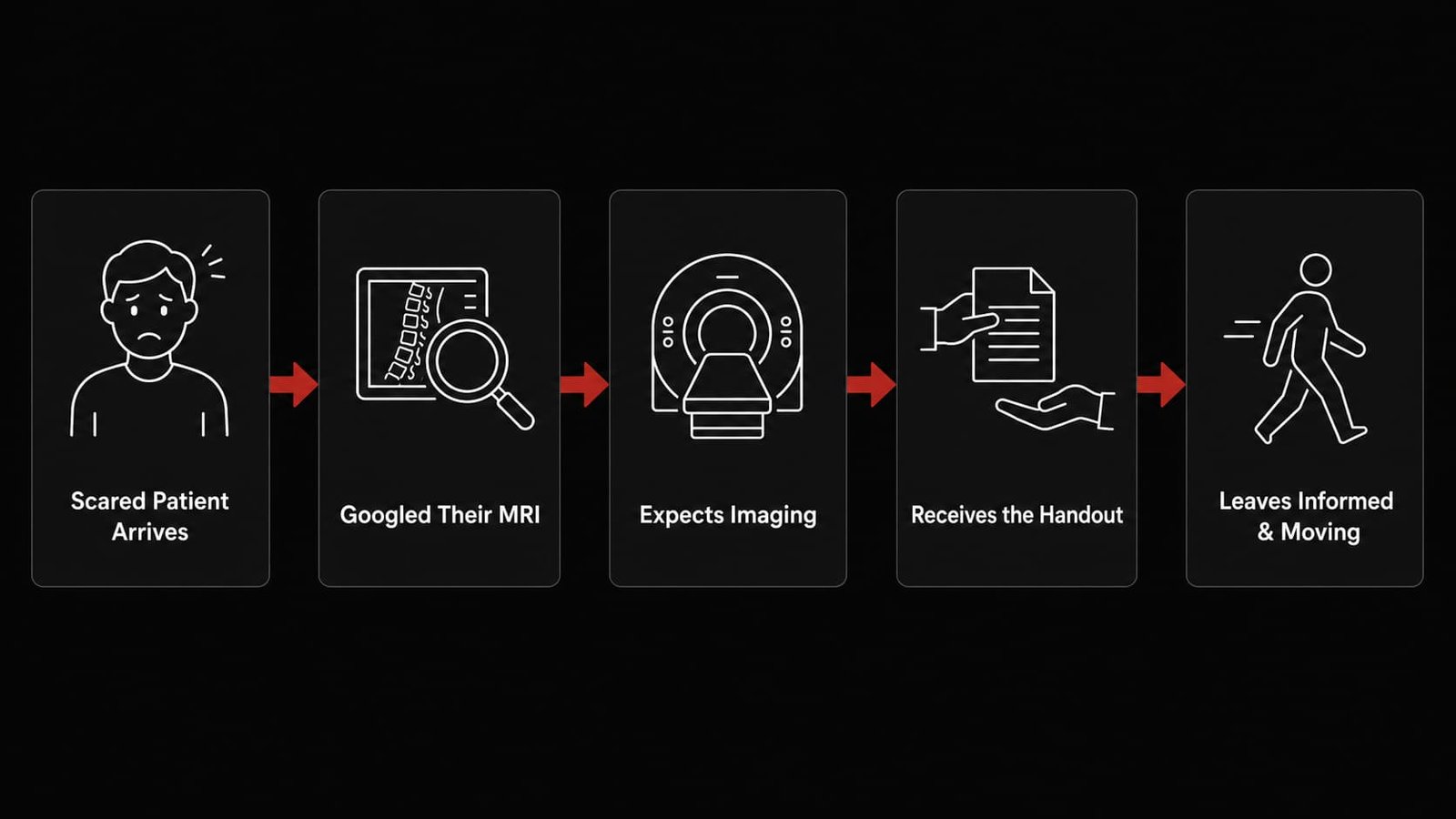
Why Your Patient Stopped Googling
The handout resets the clinical conversation before it becomes adversarial. Here is what happens when you hand it over.
Directing a Patient Out Shouldn't Create Clinical Blind Spots.
When you refer a Profile B patient to our Yorkville clinic, the clinical loop stays closed.
Clinical Correspondence
Every referral comes with a clear written summary — your records stay complete, your patient stays informed. When our assessment identifies findings beyond the MSK scope, we write directly to your practice.
Clear Boundaries
If we cannot isolate the mechanical driver within the first visit, the patient returns to you with a clear picture of why — not held in an open-ended treatment cycle.
Rapid Discharge
Once the patient has what they need, they are discharged with a clear self-management protocol. No open-ended treatment. Your patient moves on informed and independent.
Who Is Mohammad
Founder of MVMT Kinetic · Registered Physiotherapist · DPT · MScPT · 10+ years MSK clinical experience. Before referring a patient, hear directly from Mohammad — what he assesses, how he thinks, and what he measures.
1 minute 20 seconds · No production required — Mohammad speaks directly to you as a clinical colleague

"Practicing evidence-based physiotherapy — Mohammad ensures his patients understand the physiology of their presenting problem, improving the retention of the prescribed treatment. He is a knowledgeable diagnostic clinician whose dynamic personality contributes to the energy of each encounter. I recommend him most highly — he is the best."
Lunch & Learn — For Your Physician Team
If the clinical package was useful, the Lunch & Learn takes it further. A free session for your team — at your clinic, on your schedule. Typically 20 minutes.
What we cover
A practical session on lumbar triage and mechanical pattern recognition — plus the referral templates your clinic can use immediately. Typically 20 minutes — we go longer if your team wants to.
- Live walkthrough of the lumbar assessment tool with case examples
- Mechanical vs. structural pattern recognition — the five indicators that guide the decision
- When imaging helps — and when it delays recovery for your patient
- Referral templates your clinic can use the same day
- Q&A — any back pain presentation your team wants to work through